What is Astigmatism ?
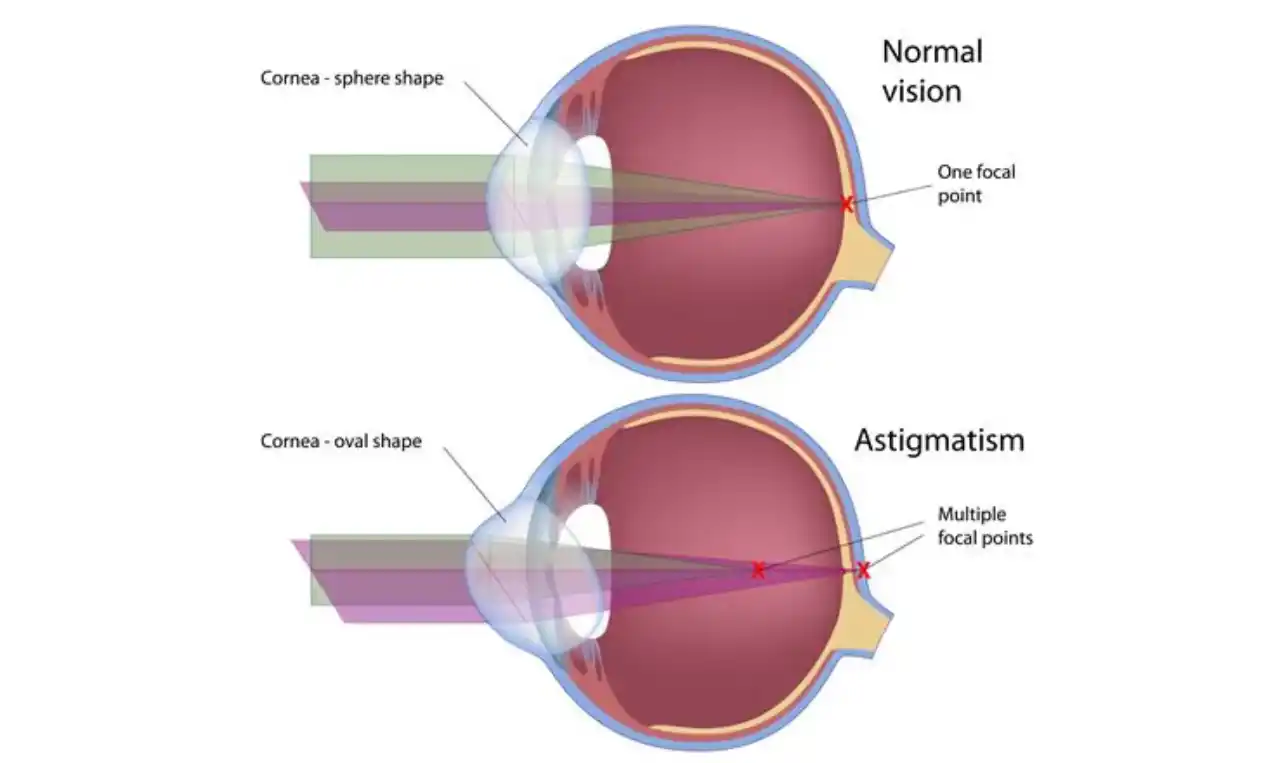
Astigmatism is a type of refractive error wherein the refraction varies in different meridian. As a result, the light rays entering the eye cannot converge to a point focus but form focal lines.
As described by Bannon and Walsh (1945), astigmatism was first mentioned in 1727 by Sir Issac Newton. But Thomas Young in 1800 published first description of astigmatism.
Refractive power of the eye is determined predominantly by variables like power of the cornea, power of the lens, and axial length of the eyeball. In emmetropia, these three components of refractive power combine to produce normal refraction to the eye.
Emmetropia is the condition where the eye has no refractive error and requires no correction for distance vision. In an emmetropic eye, rays of light parallel to the optical axis focuses on the retina. The far point in emmetropia (point conjugate to retina in non- accommodating state) is optical infinity, which is 6 meters. Ametropia (refractive error) results when cornea and lens inadequately focus the light rays. The measuring unit for refractive error is dioptre (D), which is defined as the reciprocal of the focal length in meters.
The term ametropia (refractive error) describes any condition where light is poorly focused on light sensitive layer of eye, resulting in blurred vision. This is a common eye problem and includes conditions such as myopia (near- sightedness), hypermetropia (far- sightedness), astigmatism, and presbyopia (age- related diminution of vision). A person who is able to see without the aid of spectacles or contact lenses is emmetropic.
Prevalence and distribution of ametropia vary greatly with age. Majority of children in early infancy are found to be somewhat hypermetropic. During the school years, children begin to become myopic in increasing numbers. Astigmatism change relatively little with age. The majority of children and young adults have a small amount of with-the-rule astigmatism, but in later adult years, there is a tendency for with-the-rule astigmatism to decrease in amount and for against-the-rule astigmatism to increase.
Astigmatism is divided as
Astigmatism Symptoms
- Blurring of vision: Patients with low astigmatism show transient blurring of vision, which is relieved by closing or rubbing the eyes. Eyes become fatigued with reading and the letters are described as ‘running together’.
- Symptoms of asthenopia (eye strain): Symptoms of asthenopia (eye strain) include tiredness of eyes, headache, irritability, dizziness and fatigue.
- Narrowing of eyes: Narrowing of eyes may be resorted to in cases having high astigmatism to see clear. Narrowing produces a stenopaeic slit effect which cuts down the light rays in one meridian.
- Head tilt: Some patients with high oblique astigmatism may keep the head tilted to one side to avoid distortion of image.
- Holding books close to eyes: Many patients with high astigmatism may hold the books close to the eyes in a bid to achieve larger image.
- Burning.
- Itching.
Patients with irregular astigmatism present with
- Defective vision.
- Distorted vision.
- Polyopia (seeing multiple images of a single object).
Astigmatism Causes
Astigmatism may be natural, traumatic following a wound or surgically induced as is seen following cataract surgery. Tight sutures after surgery further accentuate astigmatism.
I. Regular astigmatism may be
- Corneal astigmatism: It is due to abnormalities in corneal curvature. This is the commonest type and is usually congenital. Acquired corneal astigmatism is not infrequent, but it often gives rise to irregular astigmatism.
- Lenticular astigmatism: This is relatively less common. It may be of following types:
- Curvature astigmatism: Congenital abnormalities of lens curvature may produce small amount of curvature astigmatism. Marked lenticular astigmatism may be seen in condition like lenticonus.
- Positional astigmatism: Congenital tilting or oblique placement of lens may produce small amount of astigmatism. Congenital or traumatic subluxation of lens may also produce astigmatism of varying degrees.
- Index astigmatism: Variable degree of change in refractive index of crystalline lens of patients suffering from diabetes or nuclear sclerosis may occur.
- Retinal astigmatism: Occasionally, obliquity of macula may produce retinal astigmatism.
Optics of regular astigmatism:
In regular astigmatism, the parallel rays of light are not focused at a point but form two focal lines. This configuration of refracted rays through astigmatic surface (or toric surface) is called Sturm’s conoid and the distance between two focal lines is called focal interval of Sturm. Length of focal interval is a measure of the degree of astigmatism.
II. Irregular astigmatism may be
- Corneal irregular astigmatism: Extensive corneal scarring or ectatic conditions like keratoconus may produce this.
- Lenticular irregular astigmatism: This may be produced due to variable refractive index in different parts of the crystalline lens and rarely may occur during maturation of cataract.
- Retinal irregular astigmatism: It may be produced by distortion of the macular area due to scarring or tumours of retina and choroid pushing the macular area
Astigmatism Diagnosis
Diagnosis of astigmatism depends upon the symptoms and clinical features.
Refractive error may be determined by
- Retinoscopy: Power in two different axes may be determined by retinoscopy.
- Astigmatic fan test: Astigmatic fan test is a sensitive test to find out astigmatism.
- Jackson cross- cylinder test: Jackson cross- cylinder test helps in confirming the power and axis of cylindrical lenses.
- Keratometry: Keratometry reveals different corneal curvature in two separate meridians. Irregular astigmatism shows distorted keratometry.
- Corneal topography: Corneal topography is essential in understanding the shape and curvature of cornea, and helps in establishing diagnosis. Irregular astigmatism patients show irregularities on corneal topography.
- Very high frequency (VHF) digital ultrasound arc scanner: It is capable of obtaining 3- dimensional (3D) layered pachymetry across the central 10 mm of cornea. Resolution of scanner on cornea mode distinguishes individual corneal layers such as epithelium or stroma in all three dimensions, due to multi-meridional scanning.
- Wavefront aberrometry: Wavefront aberrometry may help in diagnosis of irregular astigmatism and the assessment of the optical quality of the eye. Simulations of the retinal images are useful to understand some of the symptoms of irregular astigmatism. With corneal topographic analysis, the origin of irregular astigmatism from the cornea or internally, or both, may be specified by aberrometry. Clinical application of aberrometry is wavefront – guided refractive surgery.
Types of regular astigmatism:
Based upon the axis and the angle between two principal meridia, regular astigmatism may be classified into:
- With-the-rule astigmatism: The two principal meridia are placed at right angle to one another with vertical meridian steeper or more curved than the horizontal one. This is called with-the-rule astigmatism, because similar astigmatic condition exists normally due to eyelid pressure on cornea.
- Against-the-rule astigmatism: The two principal meridia are placed at right angle to one another with horizontal meridian steeper or more curved than the vertical one.
- Oblique astigmatism: It is a type of regular astigmatism where two principal meridia, though placed at right angle, are not in vertical and horizontal meridian. Oblique astigmatism is often found to be symmetrical (e.g. cylindrical lens required at 30? in both eyes) or complementary (e.g. cylindrical lens required at 30? in one eye and at 150? in the other eye).
- Bi-oblique astigmatism: In this type, the two principal meridia are not at right angle to each other.
Refractive types of regular astigmatism: Depending upon the position of two focal lines in relation to retina, regular astigmatism is classified into:
- Simple astigmatism: The rays of light are focused in one meridian only on the retina. The rays of light in other meridian are focused in front or behind retina. Accordingly, it is called
- Simple myopic astigmatism: When the light rays of other meridian are focused in front of the retina.
- Simple hypermetropic astigmatism: When the light rays of other meridian are focused behind the retina.
- Compound astigmatism: The rays of light are focused either in front or behind the retina in both the meridia. Accordingly, it is called
- Compound myopic astigmatism: The rays of light are focused in front of the retina in both the meridia.
- Compound hypermetropic astigmatism: The rays of light are focused behind the retina in both the meridia.
- Mixed astigmatism: The rays of light are focused in front in one meridian and behind the retina in other meridian. Thus, eye is myopic in one meridian and it is hypermetropic in other. Such patients have relatively less symptoms as ‘circle of least diffusion’ forms on retina. It is presumed that a pencil of rays forms a minute circle of clear vision, called circle of least diffusion. Larger is the circle of least diffusion, poorer the vision.