What is Abnormal uterine bleeding ?
Abnormal uterine bleeding (AUB) is a common problem among (non-pregnant) women in the reproductive age. Formerly, it was known as dysfunctional uterine bleeding (DUB). AUB is responsible for significant health problem and social embarrassment and it is one of the common reasons women seek health care. It has a significant impact on the quality of life for the women. Women with abnormal bleeding have a lower quality of life than the general female population.
The normal length of the menstrual cycle is normally between 24 days and 38days. A normal menstrual period generally lasts up to 8days. Abnormal uterine bleeding (AUB) is bleeding from the uterus that is longer than usual or that occurs at an irregular time. (Bleeding during pregnancy has different causes).
AUB leads to loss of productivity and may result in surgical interventions. AUB is reported to occur in 9 to 14% women between menarche and menopause. The prevalence varies in each country. In India, the reported prevalence of AUB is around 17.9%.
The International Federation of Gynaecology and Obstetrics (FIGO) Menstrual Disorders Working Group has proposed to abandon the use of dysfunctional uterine bleeding (DUB), while continue to use the terms abnormal uterine bleeding (AUB) and heavy menstrual bleeding (HMB). HMB includes menometrorrhagia (excessive uterine bleeding during menstrual periods and at irregular intervals), metrorrhagia (bleeding at irregular intervals) and polymenorrhoea (more frequent periods). HMB is defined as “excessive menstrual blood loss which interferes with the woman's physical, emotional, social and material quality of life, and which can occur alone, or in combination with other symptoms.
To standardize nomenclature of AUB, a new system known by the acronym PLAM-COEIN, was introduced in 2011 by FIGO. The PALM-COEIN system is based on etiology and pathology of disorder, where PALM describing structural causes(polyp; adenomyosis; leiomyoma; malignancy and hyperplasia) and COEIN denoting non- structural causes of AUB (coagulopathy; ovulatory disorders; endometrial factors; iatrogenic; and not classified).
Abnormal uterine bleeding in women of reproductive age is a manifestation of any of a number of pathologic disorders.
Abnormal uterine bleeding Symptoms
Abnormal uterine bleeding may present as any of the following symptoms-
- Bleeding or spotting between periods
- Heavy bleeding during period
- Menstrual cycles that are longer than 38 days or shorter than 24 days
- Irregular periods in which cycle length varies by more than 7-9 days
- Bleeding or spotting after sex
- Bleeding after menopause
(Normal menstrual cycle- The normal length of the menstrual cycle is between 24 days and 38 days. A normal menstrual period generally lasts up to 8 days.)
Abnormal uterine bleeding can occur at any age. However, at menarche (around 9-14 years of age, when a girl first starts having periods) and during perimenopause (mid forties), AUB is more common.
Abnormal uterine bleeding Causes
International Federation of Gynecology and Obstetrics (FIGO) introduced PLAM-COEIN system of classification in 2011 to define the causes of abnormal uterine bleeding. There are 9 main categories of etiology of AUB, which are arranged according to the acronym PALM-COEIN.
The components of the PALM group are structural causes that can be located visually with imaging techniques and/or histopathology. These causes are polyp; adenomyosis; leiomyoma; malignancy and hyperplasia.
Polyp (AUB-P) - Uterine polyps are growths from endometrium, (inner lining of the uterus) found into the uterine cavity. These are usually benign but some may be precancerous or cancerous.
Adenomyosis (AUB-A) - This is a condition in which the inner lining of the uterus (endometrium) grows in to the muscle wall of the uterus ( myometrium). It may lead to heavy or longer-than-usual menstrual bleeding, as well as pain during menstrual cycle.
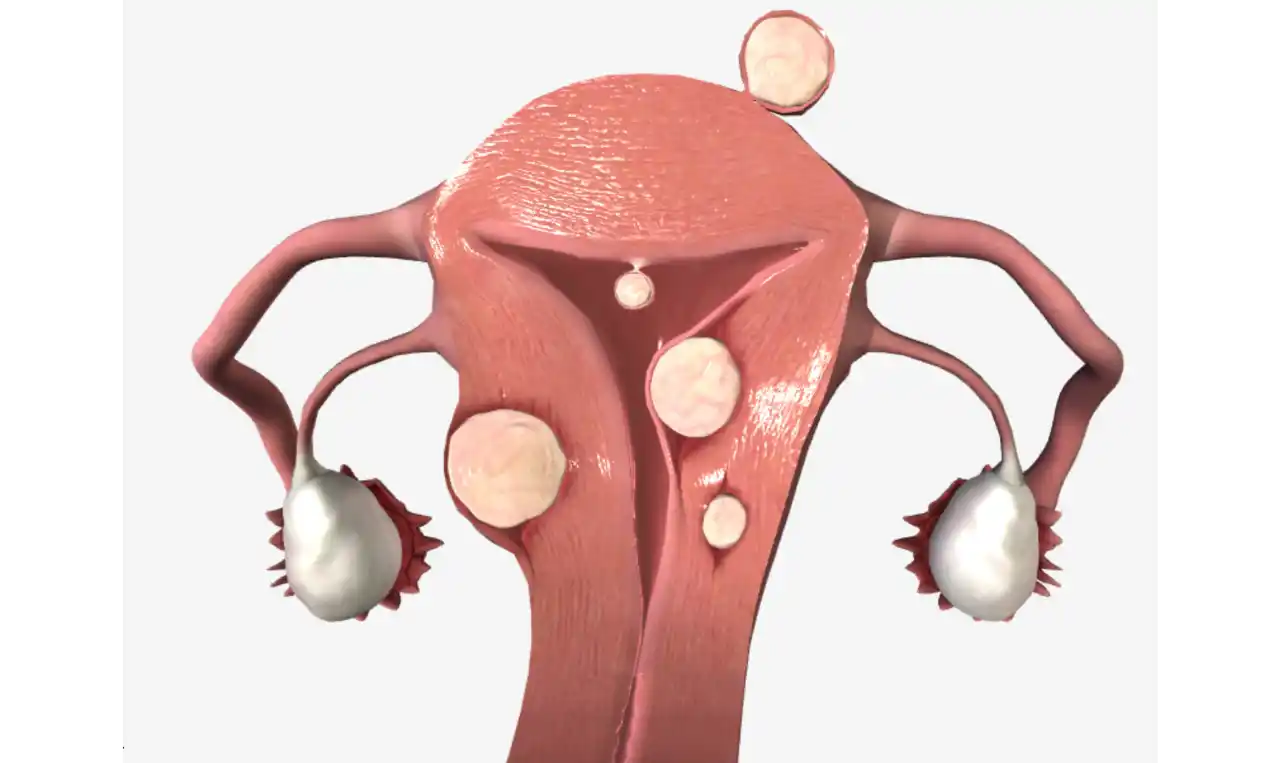
Leiomyoma (AUB-L) - These are benign fibromuscular tumors of the myometrium. Leiomyomas are known by several names, including “myoma,” and “fibroid.”
Malignancy and hyperplasia (AUB-M) - Malignancy and atypical hyperplasia are associated with, AUB and must be considered in nearly all women of reproductive age.
The COEIN group is related to non-structural causes of AUB that are not defined by imaging or histopathology. These causes are coagulopathy; ovulatory dysfunction; endometrial; iatrogenic; and not yet classified.
Coagulopathy (AUB-C)-The term “coagulopathy” includes the systemic disorders of hemostasis that may be associated with AUB. Prevalence and clinical impact of disorders of systemic hemostasis, or coagulopathies (AUB-C) (one of which, von Willebrand disease), can be identified in about 13% of women with heavy menstrual bleeding (HMB).
Ovulatory dysfunction-Disorders of ovulation may present as different menstrual abnormalities ranging from amenorrhea (absence of periods), extremely light and infrequent bleeding, to unpredictable heavy menstrual bleeding. Ovulatory disorders may be associated with polycystic ovary syndrome, hypothyroidism, hyperprolactinemia, mental stress, obesity, anorexia, weight loss, extreme exercise. Ovulatory disorders frequently occur at the extremes of reproductive age: adolescence and the perimenopause. As women approach menopause, cycles shorten and often become intermittently anovulatory.
Endometrial (AUB-E) – When uterine bleeding occurs due of the abnormalities of endometrium with normal ovulatory function, and without any coagulopathy it is known as AUB-E.
Iatrogenic (AUB-I)-Abnormal uterine bleeding associated with the use of exogenous gonadal steroids, intrauterine devices, or other systemic or local agents is classified as iatrogenic (AUB-I).
Not yet classified (AUB-N) - A category of “not yet classified” was created to accommodate entities that are rarely encountered or are ill-defined.
Abnormal uterine bleeding Diagnosis
Thorough history and physical examination are the preliminary components for diagnosing the cause of AUB, and also help to suggest investigations for final diagnosis and to guide options for management. Women with AUB may have multiple factors that may contribute in genesis of AUB or sometimes a pathology (such as subserosal leiomyoma) is present but not responsible for the AUB. In women of child bearing age, pregnancy and its related complications should be excluded.
History should include the following-
- Amount, frequency, and regularity of bleeding; dysmenorrhea (painful menstruation) or premenstrual symptoms-
o Ovulatory AUB is usually regular and is often associated with premenstrual symptoms and dysmenorrhea.
o Anovulatory bleeding is often irregular, heavy, and prolonged, which is more common near menarche and perimenopause.
- Presence of post-coital or intermenstrual bleeding
o Inter menstrual bleeding or post-coital bleeding may be the first symptoms of gynaecological cancer.
- Symptoms suggestive of anemia (such as weakness, shortness of breath with activity)
- Sexual and reproductive history ( about contraception, sexually transmitted infections, desire for future pregnancy, infertility, cervical screening)
- Impact on social and sexual functioning and quality of life
- Symptoms suggestive of systemic causes of bleeding such as hypothyroidism, hyperprolactinemia, coagulation disorders, polycystic ovary syndrome
- Associated symptoms such as vaginal discharge, pelvic pain or pressure
Examination: Physical examination of the woman having AUB includes-
- Assessment of weight, pallor, thyroid, breasts, acne, hirsutism scoring (if present)
- Abdominal palpation
- Visualization of the cervix
- Bimanual (internal) examination
Laboratory Testing-
- A complete blood count (CBC) - full blood count test should be carried out on all women with HMB to detect anaemia.
- Blood type and cross match
- Urine pregnancy test to rule out pregnancy
Tests for evaluating bleeding disorders-
- Bleeding time, platelet count, prothrombin time, and partial thromboplastin time are recommended in all adolescents and in adults with a positive history of coagulopathies.
- Testing for coagulation disorders (such as von Willebrand disease) should be considered in women who have had HMB since menarche and have personal or family history suggesting a coagulation disorder.
- Thyroid testing should only be carried out when other signs and symptoms of thyroid disease are present.
- Liver function tests
Investigations for detecting structural and histological abnormalities: Imaging-
- Ultrasonography is used in AUB cases to evaluate uterus, adnexa and endometrial thickness. Transvaginal ultrasonography may reveal leiomyoma, endometrial thickening, or focal masses.
- Sonohysterography-It is more specific and sensitive in diagnosing lesions inside the uterine cavity and endometrial hyperplasia.
- Hysteroscopy-It is an examination of the uterine cavity and the surface of the endometrium (inner lining of uterus) using a hysteroscope for diagnosis and characterization of intrauterine abnormalities.
- MRI (magnetic resonance Imaging) - MRI can be used to differentiate between fibroids and adenomyosis and for mapping exact location of fibroids while planning conservative surgery and prior to therapeutic embolization for fibroids.
- Endometrial biopsy/ histopathology- A sample of the endometrium is removed and examined under the microscope. The endometrium may be obtained during direct visualization with a hysteroscope or blindly using a sampler (a plastic tube passed through the cervix that uses suction to obtain endometrium). The purpose is to detect the pre-malignant condition of endometrial hyperplasia with cytological atypia or endometrial carcinoma.
- Computed tomography (CT)-This X-ray procedure shows internal organs and structures in cross section
Abnormal uterine bleeding Prevention
Though there are no specific measures to prevent abnormal uterine bleeding (AUB), but early diagnosis and treatment helps to prevent long-term complications, such as infertility, anaemia, hypovolemia.
Sometimes AUB resulting from hormonal changes can be prevented/ reduced by life style interventions include eating healthy diet and exercising, not smoking, maintaining healthy weight.