What is Conjunctivochalasis?
Conjunctivochalasis (CCh) is defined as the presence of redundant non-oedematous conjunctiva that may be asymptomatic, or it may be symptomatic due to unstable tear film or mechanical disruption of tear flow. It is usually found in older people and is often overlooked as a normal variant of the eye due to ageing. However, it has been seen in patients as early as the first decade of life, with an increase in prevalence and severity with age.
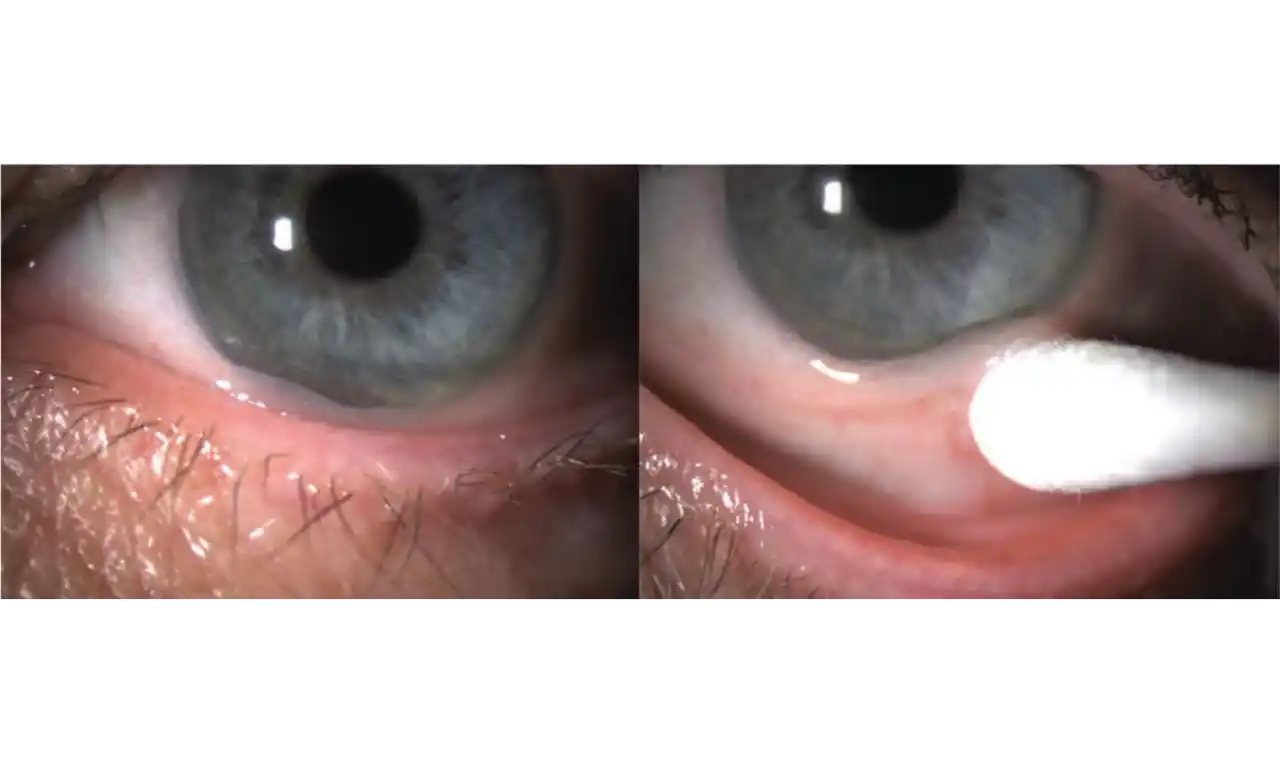
CCh is usually bilateral and consists of an elevation of the bulbar conjunctiva over the lower lid margin, most commonly in the infero-temporal region. This condition may impede tear outflow through the inferior punctum, resulting in epiphora (watering from the eyes). It may also involve the upper bulbar area with loose conjunctiva, but this is less common.
History and Terminology
Descriptions of conjunctivochalasis were noted as early as 1908 by Elschnig. Braunschweig in 1921 and Wollenberg in 1922 also described this condition. The term "conjunctivochalasis" was coined by W. L. Hughes in 1942. They described severe findings such as pain, subconjunctival haemorrhage, and exposure keratopathy. Later works described mild to moderate symptoms of CCh like dry eye and excessive lacrimation.
Other conditions causing tearing and ocular irritation must be ruled out as causative or contributory agents. Similar symptoms may be present in:
- Isolated dry eye syndrome.
- Dry eye syndrome with CCh.
- Lid diseases, e.g., blepharitis.
- Allergic eye disease.
- Autoimmune thyroid eye disease.
- Contact lens wearers.
Conjunctivochalasis Symptoms
CCh may be asymptomatic. When symptoms are present, they are non-specific and the onset is insidious. Ocular (eye) symptoms may include:
- Irritation
- Foreign body sensation
- Discomfort
- Burning
- Lacrimation or watering
- Discharge
- Blurred vision
- Dryness
- Subconjunctival haemorrhage
- Ocular fatigue
- Eye stiffness on awakening
Symptoms of CCh tend to worsen with both down gaze and digital pressure.
Conjunctivochalasis Causes
No true aetiology is known for conjunctivochalasis. Suggested causes include senile changes involving the subcutaneous, elastic, or supporting tissue in the conjunctiva. Eye rubbing, mechanical irritation, trauma to the conjunctiva, and abnormal eyelid position are also implicated.
Francis et al. suggested that the development of CCh is multi-factorial, including local trauma, ultraviolet radiation, and delayed tear clearance (Francis IC, Chan DG, Kim P, et al. Case-controlled clinical and histopathological study of conjunctivochalasis. Br J Ophthalmol 2005; 89:302-305).
Watanabe et al. showed microscopic lymphangiectasia of the subconjunctiva without any inflammation, suggesting that mechanical forces between the lower eyelid and conjunctiva gradually impaired lymphatic flow, resulting in lymphatic dilatation and clinical CCh (Watanabe A, Yokoi N, Kinoshita S, et al. Clinicopathologic study of conjunctivochalasis. Cornea 2004; 23:294-298).
Yokoi et al. found negligible inflammation in CCh patients compared to normal and inflammatory ocular surface disease samples (Yokoi N, Komuro A, Nishii M, et al. Clinical impact of conjunctivochalasis on the ocular surface. Cornea [Clinical Trial] 2005; 24(Suppl.8):S24-31).
Conjunctivochalasis Diagnosis
CCh is often under diagnosed and misdiagnosed. Non-specific symptoms and intermittent conjunctival oedema can lead to misdiagnosis. Several clinical exams may be required to confirm the diagnosis. Diagnosis of CCh is mainly clinical.
Slit lamp biomicroscopy (by an eye specialist) shows prolapsed or folds of conjunctiva in temporal, nasal, or central part of lower lid-margin. Signs include:
- Presence of redundant conjunctiva
- Altered tear meniscus
- Dryness of eyes on Schirmer test
- Reduced tear film break-up time (BUT)
- Fluorescein sodium/rose bengal dye staining in non-exposure zone
- Inferior punctum blockage in nasal CCh, resulting in epiphora
- Anterior migration of muco-cutaneous junction caused by overspill of aqueous tears
- Regional lid-margin inflammation due to overspill of aqueous tears
Patients with CCh are often diagnosed with other ocular surface diseases such as dry eye, anterior blepharitis, meibomian gland disease, or allergic eye conditions before the correct diagnosis is made.
Grading Systems
Höh et al. looked at the number of lid-parallel conjunctival folds (LIPCOF) and noted their high predictive value for diagnosis of keratoconjunctivitis sicca (Höh H, Schirra F, Kienecker C, et al. Lid-parallel conjunctival folds are a sure diagnostic sign of dry eye. Ophthalmologe 1995; 92: 802-808).
Meller and Tseng in 1998 adapted this scale to include the extent of CCh, changes with down-gaze and digital pressure, and presence of punctal occlusion (Meller D, Tseng SCG. Conjunctivochalasis: literature review and possible pathophysiology. Surv Ophthalmol 1998; 43: 225-232).
The grades of severity of conjunctivochalasis are:
- Grade 1: No persistent fold
- Grade 2: Single, small fold
- Grade 3: More than two folds, not higher than the tear meniscus
- Grade 4: Multiple folds, higher than the tear meniscus
The newest grading system proposed by Zhang et al. in 2011 further modified this approach by including symptoms (epiphora, dryness, foreign body sensation) and unstable tear film break-up time (BUT) (Zhang X, Li Q, Zou H, et al. Assessing the severity of conjunctivochalasis in a senile population: a community-based epidemiology study in Shanghai, China. BMC Pub Health 2011; 11:198). The validity of this requires further studies.
Histopathology
Most common histopathologic findings are elastosis or chronic non-granul omatous inflammation (Yanoff Myron, Sassani Joseph W. Ocular Pathology. Seventh Edition. Elsevier Saunders. 2015. P. 216.). Microscopic lymphangiectasia is typically present.
Conjunctivochalasis should be differentiated from:
- Dry eye syndrome
- Sjögren syndrome
- Meibomian gland dysfunction
- Conjunctival infection
- Conjunctival inflammation
- Chemosis of conjunctiva
- Entropion